Steep Path of “Value-Based Healthcare” Offers Indispensable Outcomes
Listen to this Article
mins | This voice is AI generated.
The healthcare industry has witnessed a gradual evolution in the past few decades. Historically, the industry has been reimbursing its providers by paying fees for the services rendered, also known as Fee-for-service (FFS) model. The stakeholders have gradually started to realize that coupling reimbursement to patient outcome & experience is the only way ahead, also known as the Value-based healthcare (VBHC) model. Moreover, legislation like the Affordable Care Act has reinforced and strengthened the VBHC model as it renders the FFS model inherently inefficient. In the FFS model, the incentive lies in providing more services, irrespective of the outcome of those services, which makes it inefficient. It is believed that the VBHC model would be an answer for the inefficiency of the FFS model.
The concept of Value-based Healthcare has evolved over the years
 The VBHC model has its roots in the Health Security Act that was introduced by President Bill Clinton in 1993 when he established a Task Force on National Health Care Reform to develop this universal healthcare initiative. It was in favor of universal coverage but used the FFS model for physician reimbursement. The proposed bill could not stand the scrutiny and it was repealed in 1994 on grounds of being too complex and costly. Later, the already established and successful ‘managed care’ model which was run through ‘Health Maintenance Organization (HMOs)’ also started failing due to a variety of reasons like reduced pharmaceutical co-pay, diminishing profitability of managed care organizations, etc. This led the Obama administration to revive the HSA by introducing Patient Protection and Affordable Care Act (PPACA) in 2010, which emphasized the use of the VBHC model for physician reimbursements. Refer to Exhibit 1 to understand the evolution of the reimbursement system in the US.
The VBHC model has its roots in the Health Security Act that was introduced by President Bill Clinton in 1993 when he established a Task Force on National Health Care Reform to develop this universal healthcare initiative. It was in favor of universal coverage but used the FFS model for physician reimbursement. The proposed bill could not stand the scrutiny and it was repealed in 1994 on grounds of being too complex and costly. Later, the already established and successful ‘managed care’ model which was run through ‘Health Maintenance Organization (HMOs)’ also started failing due to a variety of reasons like reduced pharmaceutical co-pay, diminishing profitability of managed care organizations, etc. This led the Obama administration to revive the HSA by introducing Patient Protection and Affordable Care Act (PPACA) in 2010, which emphasized the use of the VBHC model for physician reimbursements. Refer to Exhibit 1 to understand the evolution of the reimbursement system in the US.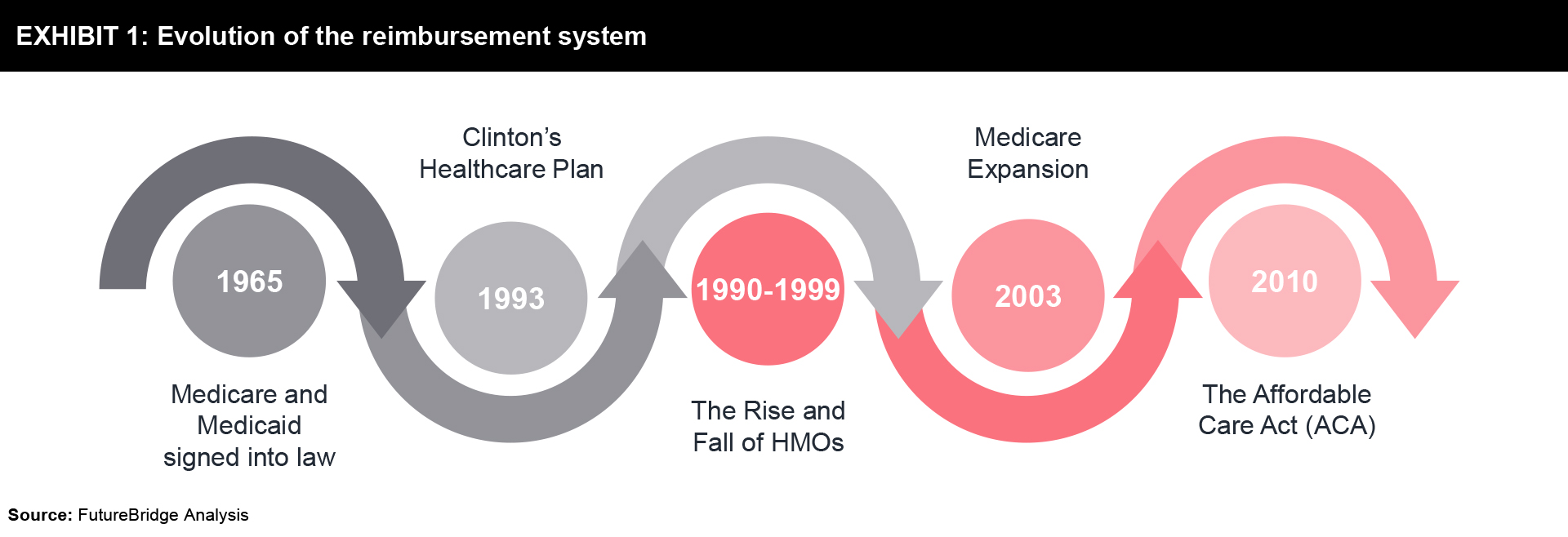
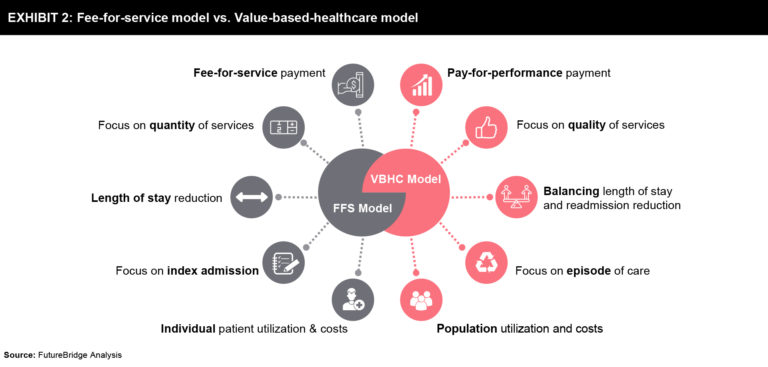
Simply put, in the VBHC model providers (including hospitals and physicians) are reimbursed based on patient health outcomes. Value-based care agreements reward providers for helping patients to improve their health, reduce the adverse effects and prevalence of chronic disease, and live healthier lives in an evidence-based way.
Exhibit 2 explains the key differences between FFS and VBHC models:
The benefits of VBHC are indispensable
- Better health at lower cost – Since the VBHC model is inherently dependent on patient outcomes, well-being and overall experience for physician reimbursement, most of the providers under this model are pro-active and try to avoid the onset of disease in its patient in the first place. Moreover, if the patient has acquired a particular disease/disorder, they also ensure that the patient recovers quickly with reduced side effects. Both, pro-activeness and quick recovery with reduced side-effects, leads to fewer doctor’s visits, medical tests, and procedures, and hence they end up spending less money on prescription medication as the overall health improves.
- Improved efficiency of providers – Rewarding providers for happy and satisfied patients acts as an incentive for them to focus more on prevention-based patients services and spend less time on chronic disease management. Moreover, they do not face the financial risk that comes along with a capitated payment system where the provider either has to compromise on the treatment provided or incur a loss when the care cost shoots up beyond the cap value.
- Increased flexibility to the payers – Since the VBHC is aimed at improving the quality of care and the overall health outcomes of the patient, it is assumed that it will ultimately reduce the number of claims giving more flexibility to the payers to offer favorable products like bundled payments which cover the patient’s full care cycle, etc. This reduces the risk exposure of both the payer and the patient.
- Alignment of medical supply prices with patient outcomes – VBHC is also aimed to rationalize the prices of the medical supply like drugs, medical devices, etc. as the final price will also be linked with the actual value it brings to the patients.
The improvement in the well-being of the citizen and reduced individual & federal spending on healthcare will ultimately boost the economy of the nation. All in all, it is assumed to be beneficial to society at large, profiting each stakeholder in one or the other way.
All kinds of Value-based healthcare models have a single goal – improving efficiencies
- Pay for Performance – Under this model, the provider receives performance-based adjustments to its FFS rates. It is a modified FFS model which incentivizes the provider with additional bonuses for meeting certain quality benchmarks and also penalizes them if they do not achieve the expected standard quality.
- Bundled Payment – In bundled payments model, providers are compensated on a “pay for episode of care” basis. An episode is defined as all the necessary services (including both inpatient & outpatient) required to treat a specific disease, disorder, or injury across the care continuum. A standard single fee covers the costs of the physicians, facility, medical supplies, etc. dedicated to a particular episode. This approach aims to improve the collaboration amongst all the stakeholders which in turn improves the efficiency to deliver superior quality service at a low cost. However, the drawback of this model is that it does not incentivize preventive care because the payment starts only at the beginning of the episode. The bundled payment rate is fixed on the average cost of an episode, hence providers can reap profits if they keep the spending below the bundled rate.
- Payment for Coordination – Also known as the ‘medical home model’, this model has a personal primary care physician assigned to each individual who looks after all the aspects of patient’s care both inside and outside the clinic. This model aims to provide superior quality and better care coordination, especially for patients suffering from chronic conditions, and to reduce hospital readmissions and emergency department visits. Similar to the pay for performance model, fixed FFS payments are paid to the provider which is then topped up with additional incentives to cover the costs of infrastructure and staff for care coordination. Providers often negotiate this incentive by demanding an FFS rate increase or a per-member-per-month payment in addition to fixed FFS payments.
- Accountable Care Organization (ACO) – ACOs are physician-led groups that collaborate to deliver high-quality care at a low cost. This model aims to ensure appropriate and timely care is delivered to the patients while avoiding duplication of services. In this model, the providers are assigned with a fixed number of enrollees and a benchmark spending target decided for those pool of members. The reimbursement to the physicians is based on FFS model during the given period, however, the actual spending is compared against the benchmark set at the end of the period and the provider enjoys a percentage share of the amount saved (positive difference). This model is flexible enough to accommodate both the one-way risk model – where providers gain for the positive difference but do not lose anything if the difference is negative and the two-way risk model – where the provider is penalized for the negative difference. Usually, in two-way risk providers are given a greater percentage share of the amount saved than a one-way risk model.
- Capitation – Under this model, a fixed amount per enrollee per month is paid to the provider irrespective of the type of treatment or services delivered. It is in the interest of the provider to treat the patient in the lowest cost setting to reap profits. The aim is to incentivize the long-term commitment to patient health and wellness with a focus on preventive care as the lesser the patient falls ill, the higher is the provider’s profit. It can be a full capitation model where it covers all the healthcare spending of the population or partial capitation where the coverage is limited to only a few services like physician services, laboratory services, etc. Since the provider is at full risk, the capitation amount is risk-adjusted to ensure they are not disincentivized.
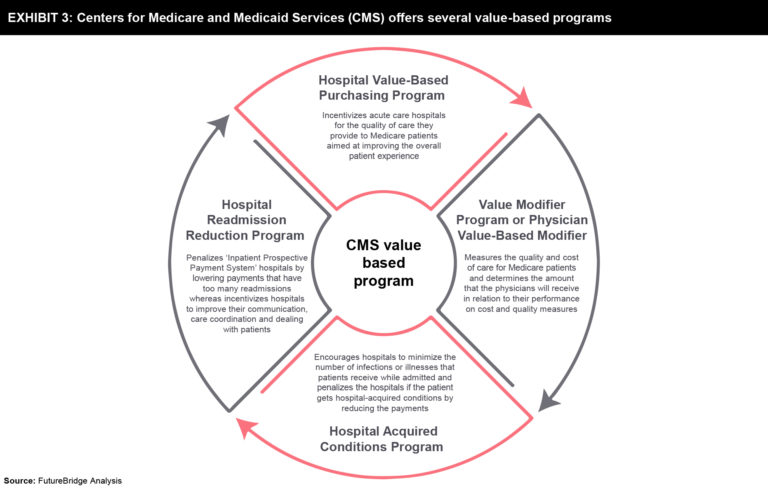
The Centers for Medicare and Medicaid Services (CMS) offers several value-based programs that are summarized in Exhibit 3.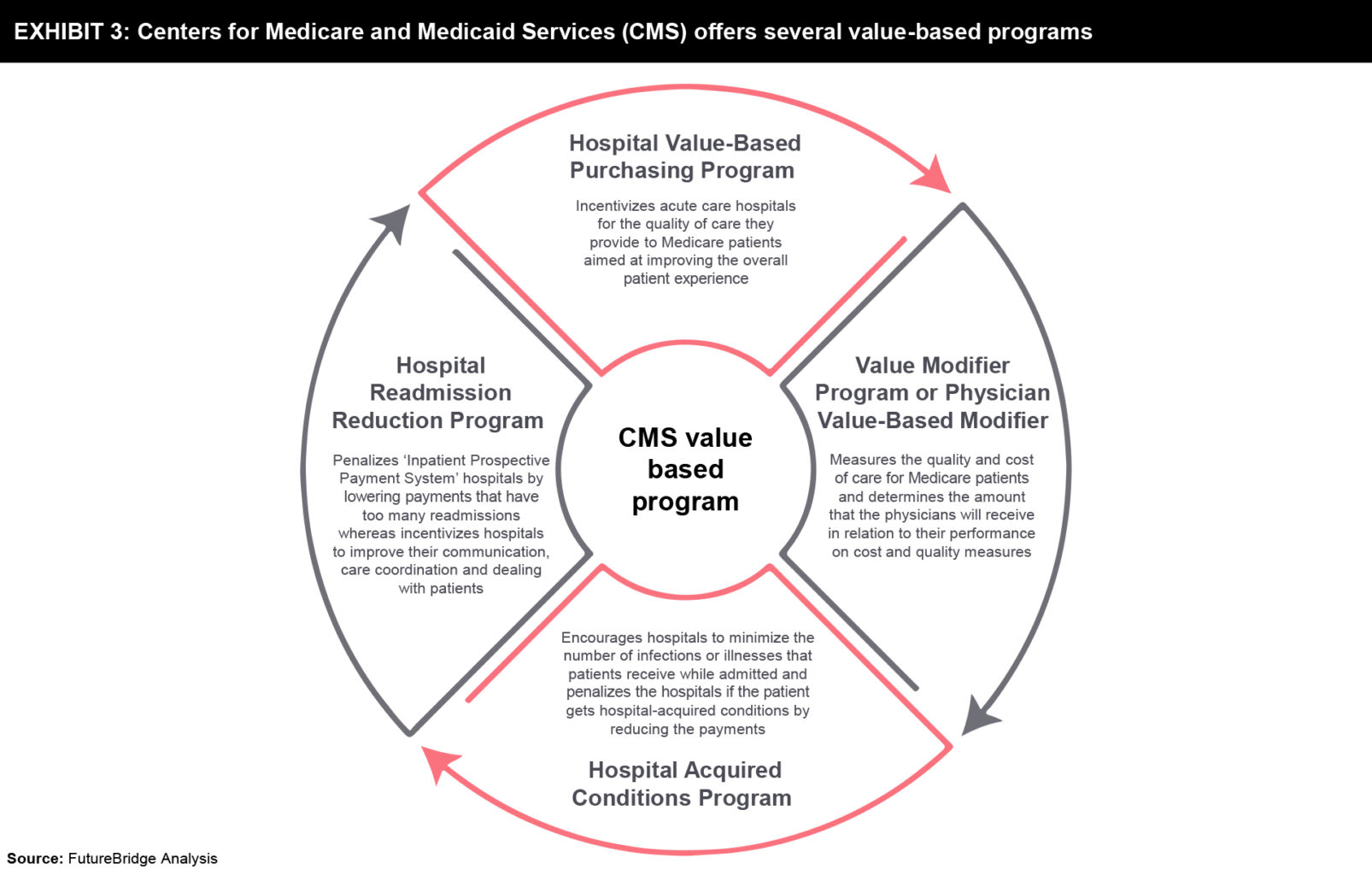
Industry examples
Though VBHC is the buzz word and it seems to benefit all the relevant stakeholders, there are very few players currently existing in the market who have deployed the VBHC model. Owing to the complexity of the model, many are running pilots to test the feasibility of the model. Refer to Exhibit 4 to understand the engagement of entities in VBHC activities.
One such example is Aetna, which has vowed to have a value-based healthcare model deployed for 75% of all claims by 2020. In 2017, the company reported that 7.2 million plan members (representing roughly 53% of the company’s claim) already received care through VBHC initiatives1.
Another example is from the medical devices industry where Medtronic is running a pilot project in Latin America. With the help of enhanced care coordination enabled by its products and monitoring system, it has been able to reduce the mortality rate related to segment elevation myocardial infarction by 30%2.
Challenges are new and deep
Though there are many challenges associated with the implementation of the VBHC model. Below are some of the key challenges faced by it:
- Defining the value of the patient outcomes & measuring performance: In the absence of clear definitions of the patient-reported outcomes, it would become very difficult to measure the performance of the care provided. Lack of standardization will lead to a lot of variations and cause reimbursement value to be influenced by biases. The industry needs to define the standards and the value associated with each patient outcome to rule out variations and biases.
- Data Integration: VBHC model requires a data lake that integrates all the data from different sources with which the patient might interact to receive a care treatment. This data lake acts as a single version of truth for the patient’s medical history. Since the existing healthcare system uses a traditional electronic healthcare record system which itself is plagued with issues like interoperability and inaccessibility, integrating such a huge amount of data to enable value-based reimbursement will be a challenge. Even if the data is integrated by using some or other technology, drawing meaningful information out of it will require special analytical capability. The shortage of skilled manpower for this task will make it even more difficult. A McKinsey study projects that by 2018, the U.S. alone may face a 50 to 60 percent gap between supply and the requisite demand of deep analytic talent3.
- Lack of infrastructure, technology adoption, and staff training: Almost all the stakeholders of the healthcare industry have adopted the FFS model and therefore have built their infrastructure that suits this model. Shifting to VBHC will require these stakeholders to overhaul their existing infrastructure and train their staff on the new model. This will be a time-consuming activity with an additional cost burden to the participants. Also, the adoption of technologies enabling measurement of outcome could be a challenge due to their reliability in absence of standardization.
Future of Value-based healthcare model
Shifting to VBHC from the FFS model is not easy and this shift might take longer than expected. The model lacks standardization and clarity in terms of the patient-reported outcomes and measuring the performance of the care provided on its basis. This has left most of the stakeholders of the industry confounded. Moreover, the lack of skilled staff is only worsening the problem. Nevertheless, as the healthcare sector is evolving, many stakeholders including physicians are acknowledging the long-term benefits associated with the VBHC model and are gradually showing their willingness to take the short-term financial hit associated with the VBHC model. However, to make it successful, the need is for the industry to come together and define & adopt the standards, develop the infrastructure and train the staff & patients. Technology has an immense role to play in the success of the VBHC model. It will be interesting to see how the industry leverages the technology to address the key issues identified and successfully implements the VBHC model which is the ultimate solution to reduce the cost curve and improve the quality of care.
References
Industry examples
Though VBHC is the buzz word and it seems to benefit all the relevant stakeholders, there are very few players currently existing in the market who have deployed the VBHC model. Owing to the complexity of the model, many are running pilots to test the feasibility of the model. Refer to Exhibit 4 to understand the engagement of entities in VBHC activities.
One such example is Aetna, which has vowed to have a value-based healthcare model deployed for 75% of all claims by 2020. In 2017, the company reported that 7.2 million plan members (representing roughly 53% of the company’s claim) already received care through VBHC initiatives1.
Another example is from the medical devices industry where Medtronic is running a pilot project in Latin America. With the help of enhanced care coordination enabled by its products and monitoring system, it has been able to reduce the mortality rate related to segment elevation myocardial infarction by 30%2.
Challenges are new and deep
Though there are many challenges associated with the implementation of the VBHC model. Below are some of the key challenges faced by it:
- Defining the value of the patient outcomes & measuring performance: In the absence of clear definitions of the patient-reported outcomes, it would become very difficult to measure the performance of the care provided. Lack of standardization will lead to a lot of variations and cause reimbursement value to be influenced by biases. The industry needs to define the standards and the value associated with each patient outcome to rule out variations and biases.
- Data Integration: VBHC model requires a data lake that integrates all the data from different sources with which the patient might interact to receive a care treatment. This data lake acts as a single version of truth for the patient’s medical history. Since the existing healthcare system uses a traditional electronic healthcare record system which itself is plagued with issues like interoperability and inaccessibility, integrating such a huge amount of data to enable value-based reimbursement will be a challenge. Even if the data is integrated by using some or other technology, drawing meaningful information out of it will require special analytical capability. The shortage of skilled manpower for this task will make it even more difficult. A McKinsey study projects that by 2018, the U.S. alone may face a 50 to 60 percent gap between supply and the requisite demand of deep analytic talent3.
- Lack of infrastructure, technology adoption, and staff training: Almost all the stakeholders of the healthcare industry have adopted the FFS model and therefore have built their infrastructure that suits this model. Shifting to VBHC will require these stakeholders to overhaul their existing infrastructure and train their staff on the new model. This will be a time-consuming activity with an additional cost burden to the participants. Also, the adoption of technologies enabling measurement of outcome could be a challenge due to their reliability in absence of standardization.
Future of Value-based healthcare model
Shifting to VBHC from the FFS model is not easy and this shift might take longer than expected. The model lacks standardization and clarity in terms of the patient-reported outcomes and measuring the performance of the care provided on its basis. This has left most of the stakeholders of the industry confounded. Moreover, the lack of skilled staff is only worsening the problem. Nevertheless, as the healthcare sector is evolving, many stakeholders including physicians are acknowledging the long-term benefits associated with the VBHC model and are gradually showing their willingness to take the short-term financial hit associated with the VBHC model. However, to make it successful, the need is for the industry to come together and define & adopt the standards, develop the infrastructure and train the staff & patients. Technology has an immense role to play in the success of the VBHC model. It will be interesting to see how the industry leverages the technology to address the key issues identified and successfully implements the VBHC model which is the ultimate solution to reduce the cost curve and improve the quality of care.
References